Just as ideas about prohibition and those who use cannabis kept it locked behind Schedule I all this time, the experiences of millions of people who have successfully used cannabis to treat a variety of conditions and who were willing to talk about it, even under the threat of prosecution, have finally unlocked the cell.
Written by
Dr. Amanda Reiman
April 24, 2026
Rescheduling cannabis is historic.
There have been no major moves at the Federal level involving this plant since it was placed in Schedule I as part of the 1970 Controlled Substances Act. You can read about what happened next here. Four months ago, the President issued an Executive Order asking for an expedited process to reschedule cannabis (a process that started under previous President Biden). On April 23rd, an order was issued by the Department of Justice to immediately move the cannabis sold through state licensed medical dispensaries, as well as any FDA approved cannabis products from Schedule I to Schedule III. Unsurprisingly, the headlines were mostly click bait with little detail, and even the take by outlets like PBS gave the glossed over version of events. So, for all you non-industry, non-lawyer people out there, here is what the news ACTUALLY means, and what comes next.
Substance Use is a Social Construct
The evolution of drug laws really comes back to the fact that substance use is a social construct. There are no “good” drugs and “bad” drugs, there is strategic messaging about the people who use drugs and the public safety risks that result from use. Of course, drugs carry varying levels of risk including chance of dependence, intoxication, side effects and how their use may impact vulnerable populations. However, from Day 1, drug laws have been designed to demonize certain groups of people at certain times in history. Cannabis was put into Schedule I not because it met the criteria (no accepted medical use, high potential for abuse, too risky to use even under a doctor’s care), but because the people using cannabis were questioning the Vietnam War and Nixon’s authority in general. The social construct of cannabis was put in Schedule I, and, once there, was very hard to remove because of the logic loop that it had no medical use, so no research was funded to look for medical use, because it had none. You can read in the article linked above that the fight to remove cannabis from Schedule I started pretty much right after it was put there, and no progress was made until Xavier Bacera called for a scientific review to consider a move out of Schedule I.
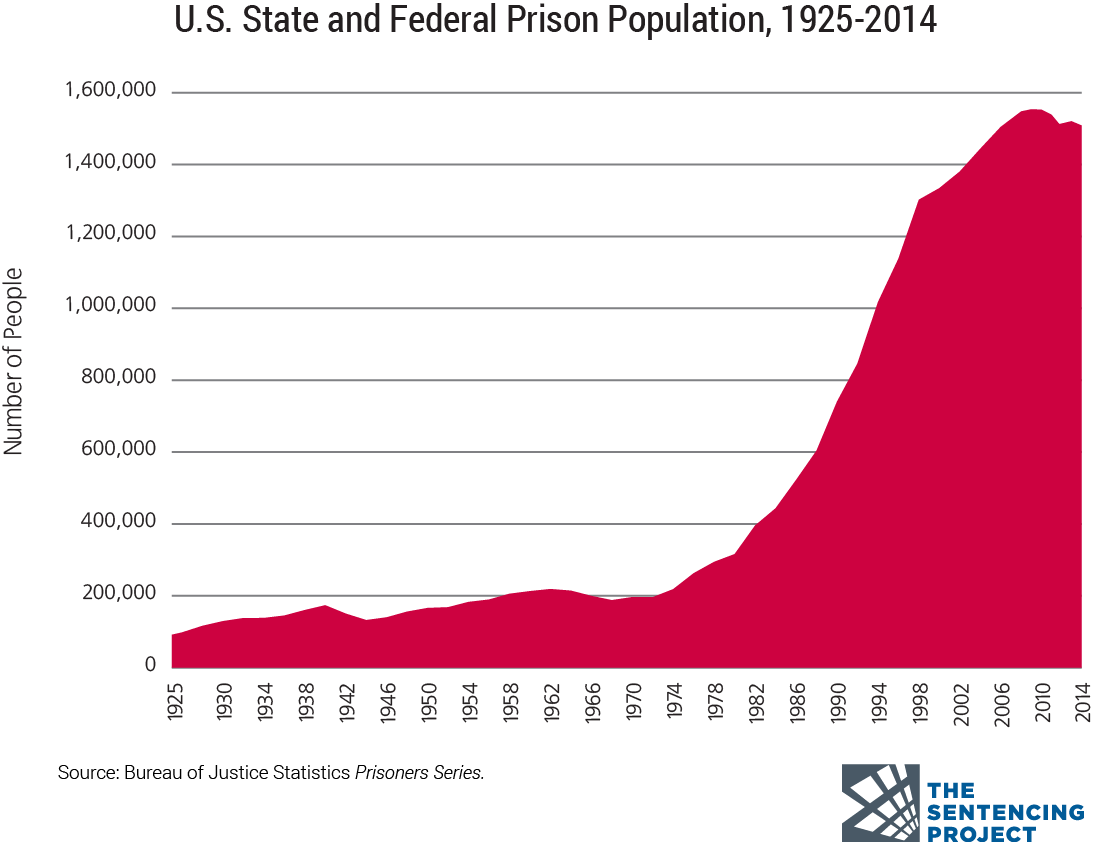
The social construct of substance use is primarily used by politicians and others as a proxy for being “tough on crime” and “of upstanding morals and values”. It can be used to send a message to voters and that they “won’t stand for that kind of reckless behavior and the riff-raff that brings it into communities.” The traditional intervention for this moral-less behavior has been the criminal justice system and incarceration. Just look at how the incarceration rates rose in the US during the height of the War on Drugs.
US Incarceration 1925-2014 from The Sentencing Project
But, I digress, this is about the Scheduling announcement, so let’s proceed.
Cannabis as a….Medicine?
The social construct idea is important because, in the absence of traditional clinical trials on humans and cannabis, its value as a medicine has been highly anecdotal and supported by an increasing number of studies into its medical utility. Traditionally, rather than science approving the use of cannabis as a medicine, millions of people are using cannabis as medicine in the face of restricted science. The belief about a lack of medical value included in Schedule I, means that there was little to no funding to investigate cannabis as a medicine, because according to the Feds, it isn’t one. So, just as the social construct of cannabis has been that of being a path to laziness and an unaccomplished life, the social construct of it as a medicine has opened doors to access. And, now the Schedule III status of cannabis feeds that construct and perhaps movement and expanded access. Some states that were hesitant to approve medical cannabis due to Schedule I may reconsider. Doctors who refuse to discuss medical cannabis with their patients may be more open to doing so. Patients who felt stigmatized for using medical cannabis may feel emboldened. These changes will not be tied to science per se, but rather the social construct of cannabis as medicine.
What Rescheduling Does and Doesn’t Do
Ok, here’s the nitty gritty, what will and will not happen as a result of the rescheduling announcement, and what may happen next? Here are the key takeaways:
Research may get easier…IF it gets funded. Conducting research with a Schedule I drug is nearly impossible. The pathways to approval can take years and a whole lot of money. Many researchers won’t even attempt it because they rely on continuous grants to keep the lights on. And, a fun little perk about cannabis, unlike other Schedule I drugs, there was a rule that cannabis for research could ONLY be obtained from one place, a grow at the University of Mississippi, which was notorious for producing cannabis that did not represent what people were actually using from dispensaries. This made research hard to generalize to the population. While that monopoly ended a few years ago, there are still very few licensed Schedule I grows, and research remains time consuming and expensive. The hope is that, with cannabis as Schedule III, not only will access to material for research be easier, but the Feds will finally start funding research on the medical benefits of cannabis using real cannabis and real people, and not mice, petri dishes and synthetic cannabinoids. Just prior to rescheduling, Democratic Representatives Dina Titus and Ilhan Omar introduced the Higher Education Marijuana Research Act, which allocates funding for cannabis research, protects universities and researchers conducting such research from federal interference, and allows researchers to access cannabis from private entities such as licensed grows and dispensaries. The President says he wants to make it easier to do research on cannabis and its medical uses, let’s see if the Feds provide the funding to support that.
Medical cannabis products are immediately designated Schedule III substances. Immediately following the April 23rd order, cannabis products sold by retailers with state medical cannabis licenses are now designated Schedule III substances. This is also the case for any FDA approved cannabis medications. Now, what does this mean? Many states stopped issuing medical specific licenses after passing adult use legalization. Instead, they passed laws designating special treatment for medical consumers, such as higher purchase and possession limits, tax breaks, and in some states, access to more potent products. The problem is, the move to Schedule III for products only applies to those sold by businesses with a MEDICAL cannabis license, not adult use. For example, in a medical only state like Florida, this would apply to all products sold, in my state of Washington, which eliminated the medical licensing system after adult use was passed, this applies to none of the products. In reality, the Scheduling designation of individual products bought by individual consumers does not really matter. One may argue that, because Schedule III drugs have an approved medical use, that Schedule III products are more “legal” than Schedule I products, but the reality is that rescheduling is NOT the same as legalization, and cannabis, medical or not, remains illegal at the federal level.
Cannabis businesses and that pesky 280E. Something that has plagued state-legal cannabis businesses for decades is 280E, the portion of the Federal tax code that disallows business deductions for anyone growing, manufacturing, testing, transporting or selling a Schedule I or II drug. Because of 280E, businesses cannot deduct standard expenses the way other businesses can, which greatly impacts their ability to be profitable. This hits small businesses especially hard because their margins are already paper thin. Cannabis “businesses” are not the same thing as cannabis “products” when it comes to rescheduling. While the status of the product may immediately move from Schedule I to Schedule III, in order to start taking deductions, a business must register as a Schedule III business and follow the designated chain of custody protocol. Let’s break down what this means. First, only those with a medical cannabis state license can register. What has not been decided is what this means for businesses that have both medical and adult use licenses and activities. Many multistate operators have business operations in medical only and adult use states, so they may have both medical and adult use licenses. Will they be prevented from registering? Will they only be able to deduct expenses related to the medical side of their business? Even if a business serves medical patients under an adult use license, they will not be eligible to register as a Schedule III business. Furthermore, we don’t yet know what the process or cost will be to register, or how long it will take and whether deductions can be taken retroactively. Additionally, according to the order, the registered businesses will have to follow the chain of custody rules outlined in the Single Convention on Narcotic Drugs, which requires the Federal government to play the role of wholesaler, effectively buying the cannabis from the licensed entity, registering it, and then selling it back to them at the same price plus a “TBD administration fee”. Again, whether this process will be achievable by smaller businesses remains to be seen. To summarize, the “opportunity” to take advantage of a reprieve from 280E may exist, but the time and money needed to do it has not been determined.
And what about adult use? The recent order only applies to businesses with medical cannabis licenses and the products they sell. This includes growers, manufacturers and others in the supply chain with medical licenses. And while there is much to figure out about businesses with dual licensing, one thing is clear, those with adult use licenses only are NOT included in this order, even if they sell products to qualified patients. A hearing has been scheduled for June 29th, to discuss the expansion of rescheduling, but there will likely be a flurry of lawsuits before then, so it truly is a wait and see situation.
What Happens Now?
Even though a lot is up in the air, movement is movement. We have been waiting for over 50 years to see cannabis moved out of Schedule I, and it is finally happening. The fact that substance use is a social construct means it is not as simple as relying on science, and that the social and political winds have more impact on where things go than what happens in a lab or clinical study. But those winds blow both ways. Just as ideas about prohibition and those who use cannabis kept it locked behind Schedule I all this time, the experiences of millions of people who have successfully used cannabis to treat a variety of conditions and who were willing to talk about it, even under the threat of prosecution, have finally unlocked the cell. While it will be a while before we really know what happens next, thank you to the activists, doctors, scientists and PATIENTS who never gave up.
Do you want to learn more about how to develop and maintain healthy relationships with psychoactive plants? Sign up for our email list for tips, stories, support and more!